Care Uk Community Diagnostics offers a coordinated set of diagnostic tests, which leads to faster and more accurate diagnoses. CAR-TOOL.EDU.VN provides detailed information about various diagnostic tools and their specifications to help you make informed decisions. Explore our site for in-depth comparisons and valuable recommendations to enhance your diagnostic capabilities. Unlock the power of effective diagnostics by leveraging quality instruments, diagnostic solutions, and innovative technologies.
Contents
- 1. Understanding the Care UK Community Diagnostics Initiative
- 2. What Defines a Community Diagnostic Centre (CDC)?
- 2.1. Key Operational Aspects of CDCs
- 2.2. Different CDC Design Models
- 3. Minimum Diagnostic Tests Offered at Standard CDCs
- 3.1. Core Diagnostic Modalities
- 3.2. Additional Optional Tests
- 3.3. Tests Unsuitable for CDCs
- 3.4. Services for Children and Young People
- 4. Implementation and Commissioning of Community Diagnostic Centres
- 4.1. NHS England’s CDC Framework
- 4.2. Financial Aspects of CDCs
- 4.3. Independent Sector Providers
- 5. Governance, Performance, and Regulatory Requirements
- 5.1. Regulatory and Accreditation Requirements
- 5.2. Performance Monitoring
- 6. Estates and Digital Infrastructure
- 6.1. Digital Connectivity Requirements
- 6.2. Unified Solutions and Innovation
- 7. Workforce Development and Recruitment
- 7.1. Workforce Strategies
- 7.2. Apprenticeships and International Recruitment
- 8. Addressing Health Inequalities
- 8.1. Data and Reporting
- 9. Enhancing Patient and Staff Experience
- 9.1. Developing Clinical Pathways
- 10. Support and Next Steps
- 10.1. Available Support
- 11. Minimum Activity Levels and Utilisation Rates
- 11.1. Imaging Modalities
- 11.2. Physiological Science
- 12. Requirements for Patient Journey Through the CDC
- 12.1. Key Steps in the Patient Journey
- 13. CDC Benefits Matrix Metrics
- 13.1. Key Metrics
- FAQ: Understanding Care UK Community Diagnostics
- 1. What is the primary goal of Care UK Community Diagnostics?
- 2. How do Community Diagnostic Centres (CDCs) differ from traditional hospital diagnostic services?
- 3. What are the minimum operating hours for a CDC?
- 4. What are the three main design archetypes for CDCs?
- 5. What core diagnostic tests must a standard CDC provide?
- 6. Are CDCs allowed to offer services for children and young people?
- 7. How are CDCs commissioned and contracted?
- 8. What regulatory and accreditation requirements must CDCs meet?
- 9. How do CDCs contribute to reducing health inequalities?
- 10. How are the benefits of CDCs measured and evaluated?
1. Understanding the Care UK Community Diagnostics Initiative
Care UK Community Diagnostics is an initiative aimed at delivering additional diagnostic capacity across England. By providing coordinated diagnostic tests within the community, patients can receive faster and more accurate diagnoses. This initiative is designed to reduce the need for hospital visits and expedite the start of treatment. As of August 2024, there are 165 operational sites, with 135 functioning from permanent buildings.
2. What Defines a Community Diagnostic Centre (CDC)?
A Community Diagnostic Centre (CDC) provides accessible diagnostic capacity, enabling patients to receive a coordinated set of tests in as few visits as possible. CDCs offer a range of elective diagnostics away from acute facilities, easing pressure on hospitals and improving patient access. These centers aim to coordinate all required diagnostic tests under one roof, ensuring a comprehensive and efficient experience.
2.1. Key Operational Aspects of CDCs
CDCs should operate at least 12 hours a day, 7 days a week. This extended availability ensures greater patient convenience and accessibility. Systems should implement plans to support CDCs in meeting this operational requirement.
2.2. Different CDC Design Models
CDCs align with three main design archetypes:
- Standard Model: Provides minimum diagnostic tests on a permanent site, along with outpatient consultations.
- Large Model: Offers all standard CDC services, plus endoscopy and other locally required services at scale.
- Hub and Spoke Model: Features a central hub (standard or large model CDC) with spoke facilities in community healthcare or commercial settings.
These models ensure CDCs meet common standards while allowing flexibility to tailor services to local needs.
3. Minimum Diagnostic Tests Offered at Standard CDCs
Standard CDCs must provide a minimum set of core diagnostic tests, covering various modalities.
3.1. Core Diagnostic Modalities
| Diagnostic Modality | Minimum Requirements |
|---|---|
| Imaging | CT, MRI, Ultrasound, Plain X-ray |
| Pathology | Phlebotomy, NT-proBNP, Point of care testing (POCT) including eGFR, pro-BNP test, anticoagulation change of dose, C-reactive protein, hCG pregnancy test, urinalysis |
| Physiological Science | 12-lead electrocardiography (ECG), Ambulatory electrocardiography (Holter, patch monitor), Ambulatory blood pressure monitoring, Trans-thoracic echocardiogram (TTE), Spot check pulse oximetry, POCT capillary blood gas assessment, Fractional exhaled nitric oxide (FeNO), Spirometry with bronchodilator response, Full lung function tests (lung volumes, gas transfer and spirometry), Field tests – 6-minute walk test, Sleep studies – multichannel home recordings, CO monitoring |
| Endoscopy (large CDCs only) | Gastroscopy – trans-nasal endoscopy (TNE) and/or oral oesophago-gastro duodenoscopy (OGD), Colonoscopy, Flexi sigmoidoscopy |
All CDC sites are expected to perform both contrast and non-contrast examinations across all tests, as approved by the Resuscitation Council.
3.2. Additional Optional Tests
Systems can consider offering additional non-core tests based on local priorities. These tests can enhance the range of services provided by CDCs.
| Diagnostic Modality | Test |
|---|---|
| Imaging | Mammography, DEXA scan, Dermoscopy, Elastography (fibroscan), CT colonography |
| Physiological Science | Urodynamics, Ophthalmology services, Audiology services, Non-complex neurophysiology (carpal tunnel syndrome) |
| Pathology | Simple biopsies (skin, breast), Other samples processed through existing pathology routes |
| Endoscopy | Colon capsule endoscopy, Sponge on a string, Cystoscopy, Flexible cystoscopy, Hysteroscopy, Colposcopy |
CAR-TOOL.EDU.VN offers detailed comparisons of various diagnostic tools, helping you understand their specifications and benefits.
3.3. Tests Unsuitable for CDCs
Certain tests are clinically unsuitable for CDC settings. This list may be updated by national clinical advisors. Examples include:
- Endoscopic retrograde cholangiopancreatography (ERCP)
- Complex interventional procedures
- Trans-oesophageal and stress echo
- Bronchoscopy and endobronchial ultrasound (EBUS)
- Cardiopulmonary exercise tests (CPET)
These tests require specialized facilities and expertise typically found in acute hospital settings.
3.4. Services for Children and Young People
CDCs are expected to offer services for children and young people where safe and appropriate. Systems must ensure all relevant governance and safeguarding arrangements are in place.
4. Implementation and Commissioning of Community Diagnostic Centres
Commissioning CDCs requires using the NHS Standard Contract. Systems can select the most appropriate commissioning and contracting model to meet local needs. This ensures no single point of failure and avoids over-reliance on one provider.
4.1. NHS England’s CDC Framework
NHS England has developed a national CDC framework of pre-qualified providers covering imaging, endoscopy, physiological science, and pathology. Commissioners can draw down services from this framework, ensuring quality and efficiency.
4.2. Financial Aspects of CDCs
The CDC Programme works closely with the NHS England Costing and Pricing team to refine the finance model for revenue allocation. Payments are based on a cost per test and payment by results methodology. ICBs should refer to NHS community diagnostic centres: Finance and contracting arrangements for 2024/25 for detailed information.
4.3. Independent Sector Providers
Independent sector (IS) providers are part of the delivery model for CDCs. Sites can be NHS-owned, IS-owned, or jointly operated.
5. Governance, Performance, and Regulatory Requirements
Governance arrangements for CDCs should reflect those of the host organization and ICB. CDCs must comply with all relevant host trust frameworks, policies, and procedures.
5.1. Regulatory and Accreditation Requirements
CDC sites must be registered with the Care Quality Commission (CQC) where applicable. They should meet accredited standards for their modalities within two years of becoming fully operational.
| Diagnostic Modality | Regulatory and Accreditation Requirements |
|---|---|
| Imaging | QSI – Quality Standards for Imaging, Ionising Radiation (Medical Exposure) Regulations (IR(ME)R, Ionising Radiation Regulations 2017 (IRR17), CQC Diagnostic Imaging Framework |
| Physiological Science | IQIPS- Improving Quality in Physiological Services (UKAS) |
| Pathology | ISO 15189 – Medical laboratory accreditation (UKAS) for the linked laboratory for phlebotomy, ISO 22870 – Point of care testing (UKAS), applied in conjunction with ISO 15189 |
| Endoscopy (larger CDCs only) | Joint advisory group on gastrointestinal endoscopy (JAG), Bowel Cancer Screening (BCSP) Programme Quality Standards, Screening Quality Assurance Service (SQAS) |
5.2. Performance Monitoring
ICBs monitor governance for all aspects of CDC delivery. Monthly diagnostic boards should be held at the system level to review governance and performance.
6. Estates and Digital Infrastructure
All CDC capital has been allocated in 2024/25, limiting further identification of new sites. Digital connectivity between diagnostic IT systems is crucial for the success of CDCs.
6.1. Digital Connectivity Requirements
Systems must ensure connected and interoperable digital services are in place within the CDC delivery model. This includes sharing imagery, clinical information, and data to support clinical pathways.
6.2. Unified Solutions and Innovation
Unified solutions should be deployed to allow centralized CDC booking and image sharing. Technology like robotic process automation can improve scheduling and reduce DNAs.
7. Workforce Development and Recruitment
Robust recruitment and retention programs are essential for developing a skilled workforce to deliver CDC services safely and effectively.
7.1. Workforce Strategies
- Use shared roles across cardiology and respiratory.
- Ensure administrative roles can schedule across all modalities.
- Utilize alternative roles like reporting radiographers and patient navigators.
7.2. Apprenticeships and International Recruitment
Systems should consider using apprenticeships to support staff recruitment and retention. A national safe and sustainable CDC international recruitment program has been developed to supply a trained workforce.
8. Addressing Health Inequalities
CDCs help reduce health inequalities by improving access to diagnostic services. Systems should ensure CDCs operate inclusively, catering to patients with disabilities and those needing interpreters.
8.1. Data and Reporting
CDCs must record all activity and report it weekly via the CDC portal. Compliance with reporting requirements is essential for effective performance management.
9. Enhancing Patient and Staff Experience
CDCs are expected to join the Experienced Based Design (EBD) Programme rollout. This involves conducting annual EBD surveys with patients and staff to gather feedback and improve services.
9.1. Developing Clinical Pathways
Systems should focus on innovation, experience, and efficiency in pathway design. Pathways should be co-developed with patients and staff, engaging relevant patient charities.
10. Support and Next Steps
CDCs are transforming elective care, providing a growing proportion of diagnostic services. NHS England and systems will monitor delivery against allocated budgets and share best practices.
10.1. Available Support
Support is available from NHS England national and regional program teams, as well as materials on the CDC FutureNHS page.
11. Minimum Activity Levels and Utilisation Rates
CDC sites are expected to perform at or above specified activity levels to maintain throughput and ensure efficiency.
11.1. Imaging Modalities
| Modalities | 5-Day Working Week | 6-Day Working Week | 7-Day Working Week |
|---|---|---|---|
| MRI – Static | 110 | 132 | 154 |
| MRI – Mobile | 110 | 132 | 154 |
| CT – Static | 165 | 198 | 231 |
| CT – Mobile | 165 | 198 | 231 |
| X-Ray | 315 | 378 | 441 |
| Ultrasound | 110 | 132 | 154 |
11.2. Physiological Science
| Respiratory Investigations | 5-Day Week | 6-Day Week | 7-Day Week |
|---|---|---|---|
| Dynamic assessments (spirometry) (± BD) | 80 | 96 | 112 |
| FeNO | 150 | 180 | 210 |
| Full lung function | 50 | 60 | 70 |
| Blood gases (capillary) | 16 | 19 | 22 |
| Simple exercise (field test) | 10 | 12 | 14 |
| Home diagnostic sleep study | 25 | 30 | 35 |
12. Requirements for Patient Journey Through the CDC
The patient journey through the CDC includes several key steps.
12.1. Key Steps in the Patient Journey
- Receive and process referrals: Develop clear referral criteria for an agreed set of pathways.
- Booking and preparation: Book patients for a coordinated set of tests, providing necessary information in advance.
- Consultation: Provide virtual or face-to-face support from a consultant specialist.
- Coordinated testing: Carry out a full range of diagnostic tests in as few visits as possible.
- Reporting: Report results in a timely manner to the referrer, offering management plan advice.
- Diagnosis and prescription: Communicate diagnosis or treatment plan directly to the patient where appropriate.
- Onward referral: Provide onward referral if needed, keeping the referring clinician informed.
13. CDC Benefits Matrix Metrics
The benefits of CDCs are measured through various metrics.
13.1. Key Metrics
| Benefit | Metric |
|---|---|
| Improved population health outcomes | Increase % of GPs with direct diagnostic referrals into a CDC electronically |
| Improved population health outcomes | Referral to scanning time for urgent referrals at a CDC is less than 14 days |
| Improved population health outcomes | Reduced time from referral to diagnostic report complete and delivered to GP/secondary care for funded pilot pathway sites |
| Increase diagnostic capacity | Number of core tests performed in a CDC: CT, MRI, echo and NOUS |
| Increase diagnostic capacity | Total number of CDC sites operational and delivering activity increases year on year of program |
| Improved productivity and efficiency | Actual activity delivered against planned capacity |
| Contributing to reducing health inequalities | Number of CDCs located in areas of deprivation: number of tests mapped against depreciation scores |
| Deliver better and more personalized service | Review of touchpoints for staff and patients detailing their experience of CDCs and whether this is positive or negative, and what learning comes from the narrative |
By understanding the Care UK Community Diagnostics initiative, healthcare professionals and administrators can better leverage its benefits to improve patient care and diagnostic efficiency. CAR-TOOL.EDU.VN provides additional resources and information to support these efforts.
Are you finding it challenging to source high-quality diagnostic tools and equipment? Do you need help comparing different options to ensure you get the best value for your investment? Contact us at CAR-TOOL.EDU.VN for expert guidance and support. Our team is ready to assist you with all your diagnostic needs.
Contact Information:
- Address: 456 Elm Street, Dallas, TX 75201, United States
- WhatsApp: +1 (641) 206-8880
- Website: CAR-TOOL.EDU.VN
FAQ: Understanding Care UK Community Diagnostics
1. What is the primary goal of Care UK Community Diagnostics?
The primary goal is to provide additional, digitally connected diagnostic capacity within communities, reducing the need for hospital visits and expediting the start of treatment. According to NHS England, these centers aim to deliver up to 9 million tests each year by the end of 2024/25.
2. How do Community Diagnostic Centres (CDCs) differ from traditional hospital diagnostic services?
CDCs offer a broad range of elective diagnostics away from acute facilities, providing quicker and more convenient access to tests. They coordinate all the diagnostic tests a patient requires, often providing them under one roof in a single visit. This reduces pressure on hospitals and improves patient experience.
3. What are the minimum operating hours for a CDC?
CDCs should provide services for at least 12 hours a day, 7 days a week, ensuring greater patient convenience and accessibility.
4. What are the three main design archetypes for CDCs?
The three main design archetypes are:
- Standard Model: Provides minimum diagnostic tests and outpatient consultations.
- Large Model: Offers all standard CDC services plus endoscopy and other locally required services at scale.
- Hub and Spoke Model: Features a central hub (standard or large model CDC) with spoke facilities in community settings.
5. What core diagnostic tests must a standard CDC provide?
A standard CDC must provide core diagnostic tests covering imaging (CT, MRI, Ultrasound, Plain X-ray), pathology (Phlebotomy, NT-proBNP, POCT), and physiological science (ECG, ambulatory monitoring, echocardiogram, etc.).
6. Are CDCs allowed to offer services for children and young people?
Yes, CDCs are expected to offer services for children and young people where it is safe and appropriate. Systems must ensure all relevant governance and safeguarding arrangements are in place.
7. How are CDCs commissioned and contracted?
Systems are required to commission their CDCs using the NHS Standard Contract, selecting the most appropriate commissioning and contracting model to meet local needs.
8. What regulatory and accreditation requirements must CDCs meet?
CDC sites must be registered with the Care Quality Commission (CQC) where applicable and aim to meet accredited standards for their modalities within two years of becoming fully operational.
9. How do CDCs contribute to reducing health inequalities?
CDCs help reduce health inequalities by improving access to diagnostic services in areas of deprivation. They operate inclusively, catering to patients with disabilities and those needing interpreters.
10. How are the benefits of CDCs measured and evaluated?
The benefits of CDCs are measured through metrics such as the increase in GPs with direct diagnostic referrals, reduced referral-to-scanning times, increased diagnostic capacity, and improved patient experience. Regular evaluations are conducted to identify areas for improvement.
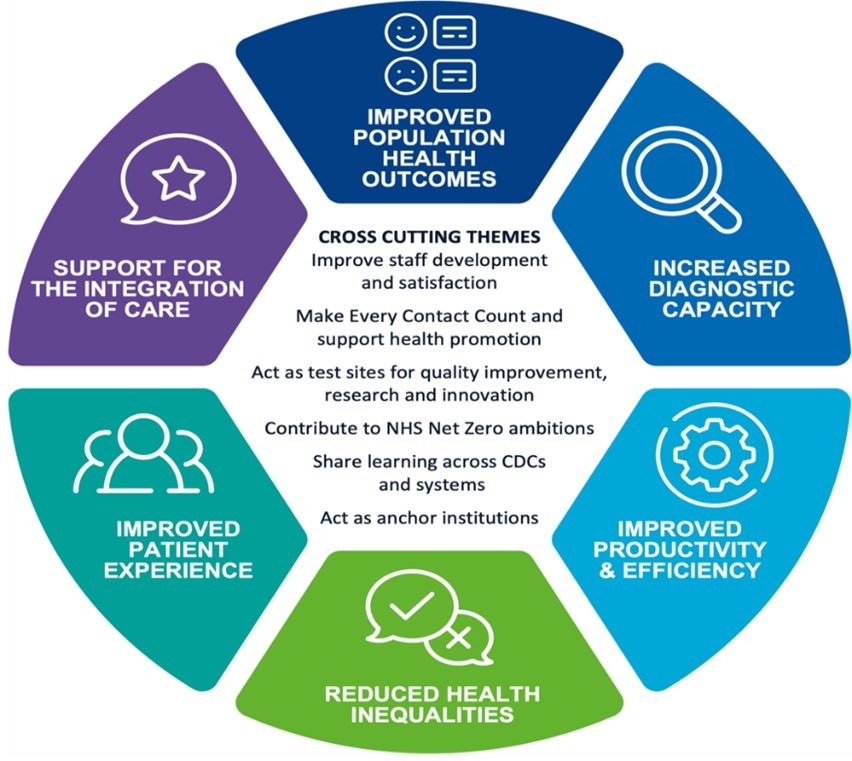 Figure 1: CDC Programme aims and cross-cutting themes. The diagram is circular and divided into six segments, each representing a different aim or theme.
Figure 1: CDC Programme aims and cross-cutting themes. The diagram is circular and divided into six segments, each representing a different aim or theme.
These FAQs provide a comprehensive overview of Care UK Community Diagnostics, helping stakeholders understand its goals, operations, and benefits. CAR-TOOL.EDU.VN offers additional resources and information to support the implementation and optimization of diagnostic services.
Do you have specific requirements for diagnostic tools or need assistance in selecting the right equipment for your CDC? Contact us at CAR-TOOL.EDU.VN for personalized support. Let us help you enhance your diagnostic capabilities and improve patient outcomes.